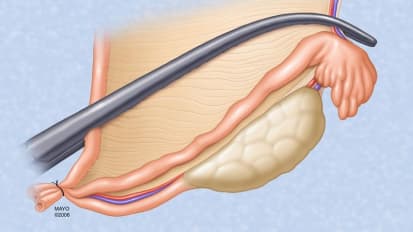
Andrew J. Barkmeier, M.D. , an ophthalmologist and retinal surgeon at Mayo Clinic in Rochester, Minnesota, repairs a relatively chronic vitreous hemorrhage. Watch as Dr. Barkmeier locates the avulsed vessel. Tearing and cheese wiring of this vessel has caused a majority of the patient's bleeding. After addressing the area of interest to see where the tear is extended, Dr. Barkmeier amputates the affected vessel.
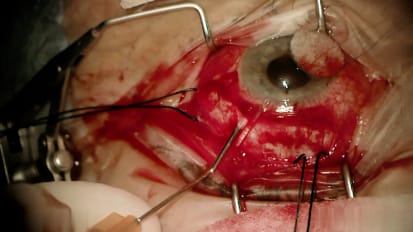
Mhm. So here we are making our incision 30° angle to the square era. So we're cautiously going to the central vitreous. We can see that there's some dehumanize globalized hemorrhage. We scrutinize the B scan ultrasound beforehand and there's an area of traction visible at About 2:00 interior early. So now we'll slowly go around 360° counterclockwise. And now we've separated all of the vitriol retinal traction there at this point where moving the infusion to direct it posterior lee, basically, we want to finish our peripheral the trek to me and then we'll probably go down with a soft tip to remove it. And then we'll then we'll be able to see if it's actively bleeding. So at this point we are shaving the peripheral vitreous skirt, we're rotating the eye far in the direction that we're working. So we can see here that we have an evolved vessel that is tearing and cheese wiring of the of the vessel that's caused probably the majority of this bleeding. We have a tear here that will need to surround. So now we'll address this area of interest here. I want to see where the terror is extended. Just amputate this area actually. So at this point we're using scleral depression to shave the vitreous space for two primary goals. One is to improve our view too, become confident that we've excluded any potential retinal tears. and number two is there's less hemorrhage remaining in the eye that will enter the vitreous cavity post operatively and blurred his vision. No, just perform some ender laser surrounding the break. So at this point we'll remove the ports and we'll have a very low threshold to suturing the ports anytime. There's a and vascular issue where hemorrhages possible. I want to reduce the risk of of hipaa Tony causing vitreous hemorrhage post operatively.
Related Presenters