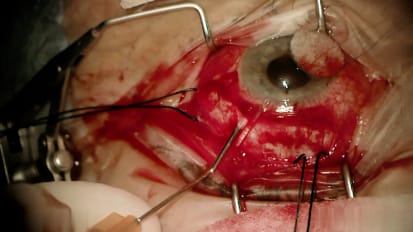
Andrea A. Tooley, M.D. , an oculoplastic and orbital surgeon at Mayo Clinic in Rochester, Minnesota, performs a bilateral upper lid blepharoplasty with a bilateral Mullerectomy ptosis repair. Dr. Tooley's patient had moderate ptosis with good levator function and a good response to phenylephrine in clinic. Watch as Dr. Tooley performs this straightforward upper eye procedure at Mayo Clinic.
So we're just making our upper lid incision here with the 15 blade. So the same thing here. Making our incision in our lower left crease to start after we make our incision we'll take off the upper eyelid skin and articulate varies. So now he's monopoly Kateri to cauterize our incision. So you can see kind of this nice bed here. It's basically almost all still or vehicular various. So I will go in and take a little strip of orbit again. I'm gonna go ahead and target that nasal fat pad now and remove some of that two D. Bulk for him. The nasal fat pads pretty sensitive. And so I do tend to give it a little extra local and excise this nasal fat pad here and I just use a combination of cut and co ag on the coterie to excise it. It can be vascular. So and you don't want any bleeding post septal in the orbit. Right. I'm just gonna take off that little strip of or bic centrally. So we're going to target that nasal fat pet over here again. Alright so we're gonna flip the lid. But we're going to market in three spots nasal central and lateral. Now we're gonna place our silk traction suture. So now we have our three loops on each side and those are going to be our three attractions. What I want to do is I want to come over and you want to center this on the tarsus nice and we just lock that in place. So now I just cut the loops. So I'm gonna start my suture up in the lid and I'm gonna exit posterior to the clamp lateral or medial. It doesn't really matter because I like to go back and forth. Okay, so now we have forehand and backhand it and we weave it across the lid. So this is kind of a trickier part. So then I do my reception and you don't want to cut your future. So you just came up and metal on metal the whole way across. So now I like to close the cons. You definitely don't have to close the cons but I feel like it helps with homeostasis. So now we enter in our incision and will externalize our needle. So the same thing over here, we're just gonna mark the lid on easily centrally and laterally and the same exact thing we're going to come down over and we want it centered on our tarsus. Yeah, I like the look of that very much and we're just going to do the same thing we did on the other side, right under our clamp and then we'll do our reception and now we'll weave it back and close the cons so that our wound is closed. We'll go into our wound and come out close to where we entered. Alright, we're gonna close the lids now
Related Presenters