Mayo Clinic otolaryngologists Garret W. Choby, M.D., Jamie J. Van Gompel, M.D., and Kathryn M. Van Abel, M.D., demonstrate the resection of an esthesioneuroblastoma by a combined nasal endoscopic and open craniotomy approach.
Garret W. Choby, M.D.
Jamie J. Van Gompel, M.D.
Kathryn M. Van Abel, M.D.
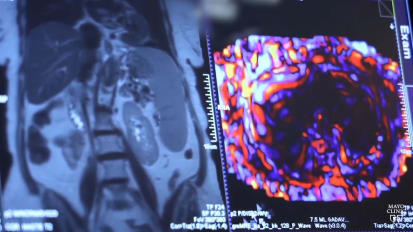
This is Garrett Choy. And today, we will be discussing a combined open and endoscopic cranial facial resection for anesthesia neuroblastoma. Here is the patient's imaging studies. You can see he has a fairly extensive estes neuroblastoma, um primary involving the left side of his nose, but also crossing midline. And what you'll see on this Saul MRI scan is that there's quite a bit of dural nodular enhancement that crawls up the poster table to his frontal sinus nearly to the apex. So, in this particular case, we elected for a combined open and endoscopic approach in order to maximize our exposure to the poster table, the frontal sinus where this involved dura was. And as you'll see later in the case, there's also extensive involvement of the mucosa, the frontal sinus, the up to the apex of the frontal sinus, which this uh combined open approach really allowed us to get excellent access to. And here is my neurosurgery partner, Dr Van Gumpel, beginning with the bifrontal craniotomy. You can see a Ronal incision being carried out there in the scalp flap, uh being raised. In this case, we are leaving the cranium uh down onto uh the cranium itself and we'll raise that as a separate flap uh just here in a moment. This allows for a very nice robust uh reconstruction option. When you're doing a combined open and endoscopic approach, you can see here. Now, after that, the skin has been, has been raised. Uh an incision is made out in the pericranium to allow us to raise that uh interiorly again, peta on our super orbital and super trochlear vessels as you can see here. And the next thing we're gonna look to do is go ahead and access uh the craniotomy just above our frontal sinus as you can see this particular case. So here are some burr holes being carried out as we enter into this area. After the osteotomies have been completed, uh we then go ahead and raising and, and uh removing that bone flap as you can see in this image dura is then uh being exposed as you can see here and then we'll incise into the dura here momentarily again, because of all that nodular en hands crawling up the post your table of the frontal sinus to its apex. We're gonna go ahead and start by removing some of that Durra in this particular case, just above there, in order to access this area and remove that portion of the patient's disease. In this particular case, uh we will end up cranials, the patient's frontal sinus. So as you work through this area and uh address and remove the post to your table of the frontal sinus. We're going to of course, remove this area for uh disease control and tumor resection. It's also very important that the entirety of the mucosa of the frontal sinus is completely removed to reduce his risk of postoperative mucocele formation uh or leading to other infectious ideologies. We of course sampled that uh mucosa as well in much of that frontal mucosa was involved with tumor up until again, the apex of the frontal sinus uh which again was nicely accessed through our open uh bifrontal craniotomy. Here we are now turning our attention to the intranasal portion of the case. What we'll do first is track and map out the tumor. I think it's very important to debulk the tumor that is freely hanging in the nose without any mucosal attachments, especially the area towards the nasopharynx. What that is going to allow for is uh egress of blood into the nasopharynx allowing that uh egress port if you will, in order to improve your visualization throughout the case, a large portion of the tumor has been taken already uh for uh permanent uh section pathology. And we'll debulk this lower portion of the tumor with a micro breeder. As you can see here, this portion that is simply free flow in the nasal cavity without any mucosal attachments. Here's that last bit of tumor in the nasal pharynx, uh being removed again to allow uh more ready access for egress of blood flow. Throughout this case with this vascular tumor, we're now tracking it up onto the nasal septum. As you can see here in the area of the patient's middle turbinate because the bifrontal craniotomy has already been completed. We'll be able to uh access that area readily and see that. Uh In short order, you can see here, tumors free from the lateral nasal wall in the area of the inferior t terminate towards the area of the max sinus. We'll take out the rest of the left middle turbinate, as you can see here, uh as tumors involving it. And when dealing with sin, nasal malignancies from an endoscopic standpoint. Again, the the key parts with tumor dissection are to debulk those areas that are freely hanging and then closely assess the mucosal areas that it's attached to and then take wide margins around this. So as you can see here, I'm using a needle tip, Bobi Cotter in order to incise wide margins around the nasal septal involvement, as you can see here and then we'll sample all these areas uh for margins as we resect this this area. Here we are poster nasal septum uh making army coastal incisions. Then coming the whole way through the septum on the contralateral side. There is some tumor involvement in the high superior septum on his right side as well. But here we are making those mucosal cuts on the left side and then performing our septectomy. And what I typically like to do is then sample the margin on the side left in the nasal cavity. So we resect the area of the uh tumor itself, then we'll sample the, the mucosa on the side that's left in the nasal cavity. So just for some examples, here's uh in sizing and checking our uh left inferior septal margin as well as an anterior, inferior septal margin. And I like to be very careful with these as I label them to ensure I know exactly where in the nasal cavity they came from. So in case anything comes back positive, we can easily go back and track that. Here we are uh making our incisions on the lateral nasal wall again, uh fairly sense of involvement here in the lateral nasal wall. So we'll make our incisions and then take our margins uh adjacent to it. I prefer a needle tip, Bobi Cotter. Although other things can be utilized here including a cole elevator or other cold steel instruments. Um obtaining and tracking the margins on the intranasal side is a very important part of this surgery. Here, we are coming through and marking on the contralateral side and then making corresponding incisions in the patient's right side of his nasal cavity. Uh Again, we'll make our incisions here and we'll take out that septum, but then we'll mark out and take our right sided margins as well. Uh In short order, as I mentioned, earlier, uh a large nasal septal flap is not possible in a case like this due to tumor involvement of it. So, in these cases, even if you would choose a purely endoscopic cranial face resection, a pericranial flap would likely be needed for our reconstruction. However, in a case like this, where we're doing a combined open and endoscopic approach, uh the pericranial flap is already raised and accessed and will drop that in from above. Uh for our reconstruction. Later on here, we are outlining the mucosal incisions again, for our right sided mucosal incisions of the nasal septum. And then we're gonna go and take out all that bone and cartilage and complete our septectomy. The most important thing in these cases is to completely remove the tumor and obtain and obtain negative margins. So, if you think about these tumors from a philosophical perspective, uh certainly there are different tools to do that. There's purely endoscopic approaches. There's combined approaches and there are purely open approaches. But the bottom line is the approach you select should really be dictated by the tumor and what you're most comfortable with obtaining complete tumor resection. Here we are on the right side, uh completing unsin toy and we open the max sinus uh for long term surveillance. Although the tumor is not directly involved in that area, we were also anticipating that he will receive adjuvant radiotherapy, which can cause uh scarring and chronic sinus problems in many patients So this is also helpful to uh prevent that long term. Here, we are now opening up the sphenoid sinus. As you can see here, I like uh up to Mike for a lot of uh the, the work back here towards the sphenoid. What you can see here is that uh sphenoid mucosa looks very normal. Now, we will also sample the areas around here to ensure it's negative as well before chalking up to being normal, but certainly has a normal clinical appearance uh in the sphenoid sinus. Now, here we are back on the left side, you're seeing the left nasopharynx there with our uh lower septectomy defect, which will all come out here in a few moments and looking to the contralateral side as well. And again, we'll make some incisions here in order to fully remove uh all of the mucosa uh in this area. We again sample margins as we work through this area as well. Of course. And here we are completing our septectomy, bringing that bony post, your septum off the roster of the sphenoid and removing that in it entirety and then bring our kerosene up again in the area where we've made our mucosal cuts and incisions uh in the more anterior septum to resect that in its entirety as well. There you see the rest of the septum coming out of the nose and just completing that uh inferior portion as well. Now, here we are working on the lateral nasal wall. We're over top of the nasal lacri mole duct in this particular shot. As you can see here, we have already taken margins anteriorly and here we are peeling all the soft tissue off of that area. As I mentioned earlier, I'll go ahead and complete uh a max and open the on this side as well. You can see that area, the max sinus is secondary obstructed and there's uh eco appearance in that particular area. The mucosa there is inflamed, although not directly involved with tumor. And we of course, took uh samples of it to ensure that as well uh during the surgery and I'll keep working here on the lateral nasal wall, uh take this mucosa as it transitions from uh the lateral wall over top of the nasal lamont and towards the orbit. What you can see here is that carefully peeling uh all this mucosa out over this area and being to expose the bone uh of the uh la pa and the nasal Lamo duct. And here we are opening up the left sphenoid sinus. Again, you can see there's a lot of post obstructive secretions within the sinus. Uh Although the sinus itself was not directly involved, we of course sampled that mucosa as well. Uh But it was negative, you just caught a glimpse of the cran from above in A T coming through in that particular area. I will note that uh the interior post er arteries have already been cauterized from above and bilateral factor bulbs have already been resected because a large portion of this bone was exposed, although not directly involved with tumor, I thought it would be prudent to go ahead and drill down the entire, to kill the rostrum. To remove that. I find in many patients that have exposed bone following the surgery and undergo adjuvant radiotherapy, that area has a tendency to crust long term and can cause problems with osteoporosis. So I do like to remove the bulk of that bone whenever possible in order to help to prevent some of those uh side effects of radiotherapy. Now, as you look at the nasal cavity, you'll see obviously a much uh wider view there with the septum gone and the cranial base gone. I'm now taking down the limit of pare in order to expose the periorbita on the patient's preoperative scans. Uh the tumor certainly a butted the orbit this area, there is no clear intraorbital extension. So in these cases, what I typically do will uh be remove the entirety of the limit of pasha and then remove and sample the per orbit itself to see if it's involved with tumor. If it is involved, we may, we may go ahead and resect out the entirety of it if it's clean. However, we'll typically leave the remaining portion of the per orbit in place. I like to maintain that plane uh right along the per orbit to make sure this fat stays intact to make sure your biopsy does not inadvertently get uh the media erectus, the period orbital was free of tumor in this case as well. And then again, I, I, I think it's prudent in these particular cases where the tumor abuts the nasal lac duct system to go ahead and drill down the entirety of the lac system and then sample uh the lac sac and the uh other soft tissue contents in the lacri mole system to which ensure it's not involved with tumor. So here we are uh drilling down the lac mole system and using a tumor and take the rest of that bone down there. We are entering that mucosa over top of the uh as you can see there and we'll go ahead and sample that mucosa uh for frozen section pathology. As I mentioned earlier in this particular case, this came back a negative uh for tumor involvement. However, I do think it's really important to be extensive in these cases. I'd much rather open up someone's lack mole system and deal with a pier later on than to leave tumor there uh during their resection. In my experience with radiotherapy, many of these patients will end up uh scarring down their lack mole system and may require DC R S down the road I have in the past uh stented this system prophylactically. But typically, what I'll do nowadays, I'll, I'll let them uh get the radiation and heal from that. And then we'll consider uh doing a DC R down the road. Here, I am just drilling down the frontal beak as you can see here, uh ensuring that there's no further mucosa in that particular area and just visualize this area better for reconstruction and for long term surveillance. Now, we'll go ahead and get a combined look uh both through the nose and from above, after the tumor has been resected and we've uh achieved our negative margins. We are beginning to think about our reconstruction. Here, we are just drilling down smooth uh again, that into your table, the frontal sinus in uh making sure that our flap is gonna lay down there uh very nicely on top of smooth bone. Here is one of the final views endoscopically prior to reconstruction, you can see both pheno is there and the planum uh we're section with Teela from above to our c atomy defect. And then uh what will become our new neo frontal sinus after cran for our typical reconstruction for cases such as this, what we like to do is to use our facial la as a primary closure as a patch in the dura which is sutured to the dural defect. We then will lay in our pericranial flap covering the entirety of the cranial base from planum uh to uh the remnant interabled the frontal sinus in orbit to orbit and then reinforce some of those edges with additional fascia lata as needed. After we're satisfied with our reconstruction, I'll typically put some absorbable packing material in the nose in cases like this where uh there's very little support in the nose and the majority of intranasal contents have been resected. I will typically place some mirror cells as well. In this case, we placed uh four gloved mirror cells underneath our packing to have nice support in that area. And here is the patient's postoperative uh MRI scan. As you can see here, he's undergone an extensive uh resection, creation, the frontal sinus and then reconstruction with a uh peral uh flap as well as fashion autograph. As you can see here with the uh neo dura laid up there. And here is him postoperatively uh about a month or so after surgery, things have been uh opened. He's been uh Debre and you can see some crusting there along that uh Perran graft, which happens in most of these cases when considering CYA malignancy resection such as aesthesia neuroblastoma. In many cases, we are able to complete this with a purely endoscopic Antero based rec section. However, the extent of tumor will dictate the approaches needed in a case such as this with extensive dural involvement along the poster table, the frontal sinus and frontal sinus mucosa itself. We elected for a combined open and endoscopic uh approach. This allows a bit better access for tumor removal as well as uh nice reconstruction with a Perran flap when things like a septal flap are not available for reconstruction. The most important part of considerations for these cases is a complete resection of tumor with negative margins. And selection of the approach is dictated by what will give you the greatest chance of achieving that long term surveillance is needed. And many patients will also go on to receive advent therapy such as radiation or in slut cases, chemotherapy.