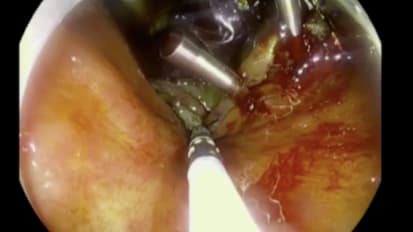
David L. Diehl, MD demonstrates how the DiLumen™ double balloon platform can effectively reduce sigmoid looping and shorten the colon, improving reach and control during complex polypectomy procedures.
Related document: Colon Shortening Technique
Related Presenters
David L. Diehl, MD is a board-certified and fellowship-trained gastroenterologist. His clinical interests include endoscopic ultrasound, endoscopic retrograde cholangiopancreatography (ERCP) and innovative advanced therapeutic endoscopy. ...
Related Videos