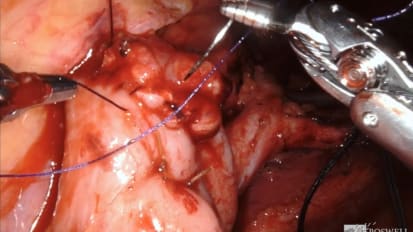
Day 2 (part 1 of 3) of the Masterclass on Bladder Cancer at the Roswell Park Comprehensive Cancer Center featuring a robot-Assisted Radical Cystectomy with Pelvic Lymph Node Dissection and Intracorporeal Ileal Conduit. This includes a panel discussion with Peter Wiklund, MD, Mount Sinai Health System; James Peabody, MD, Henry Ford Health System; Karim Chamie, MD, University of California; and Bernard Bochner, MD, Memorial Sloan Kettering.
Related Presenters

Chair, Department of Urology
Director, Robotic Surgery
Director, Applied Technology Laboratory for Advanced Surgery (ATLAS)
Robert P. Huben Endowed Professor of Oncology
Professor of Oncology
Khurshid A. Guru, MD, was appointed Director of Robotic Surgery at Roswell Park Comprehensive Cancer Center in October 2005. Dr. Guru completed his residency training in Urologic Surgery (2005) and a Robotic Surgery Fellowship (2004) at ...
Related Videos